Clinical Research & Literature — Cardiology
Blood Pressure Monitoring
Blood pressure monitoring can help with diagnosing and treating this condition.

Clinical Research & Literature — Cardiology
Blood Pressure Monitoring
Blood pressure monitoring can help with diagnosing and treating this condition.
Office blood pressure monitoring
Auscultatory or oscillometer semiautomatic or automatic sphygmomanometers are the preferred method for measuring BP in the doctor’s office. With inadequate attention to the standardized conditions recommended for the valid measurement of office BP, it can be performed improperly. Improper measurement of office BP can lead to inaccurate classification, overestimation of a patient’s true BP, and unnecessary treatment.²
Masked Hypertension³
The addition of ambulatory blood pressure monitoring to conventional clinic measurement for defining blood pressure status in clinical practice has added a new complexity to the process. The separation of normotension and hypertension can be assessed independently by each of the two methods. We thus have four potential groups of patients who are, first, normotensive by both methods (true normotensives); second, hypertensive by both (true, or sustained, hypertensives); third, hypertensive by clinic measurement and normotensive by ambulatory measurement (white-coat hypertensives); and fourth, normotensive by clinic measurement and hypertensive by ambulatory measurement (masked hypertension). In this paper the importance of this fourth group will be addressed.
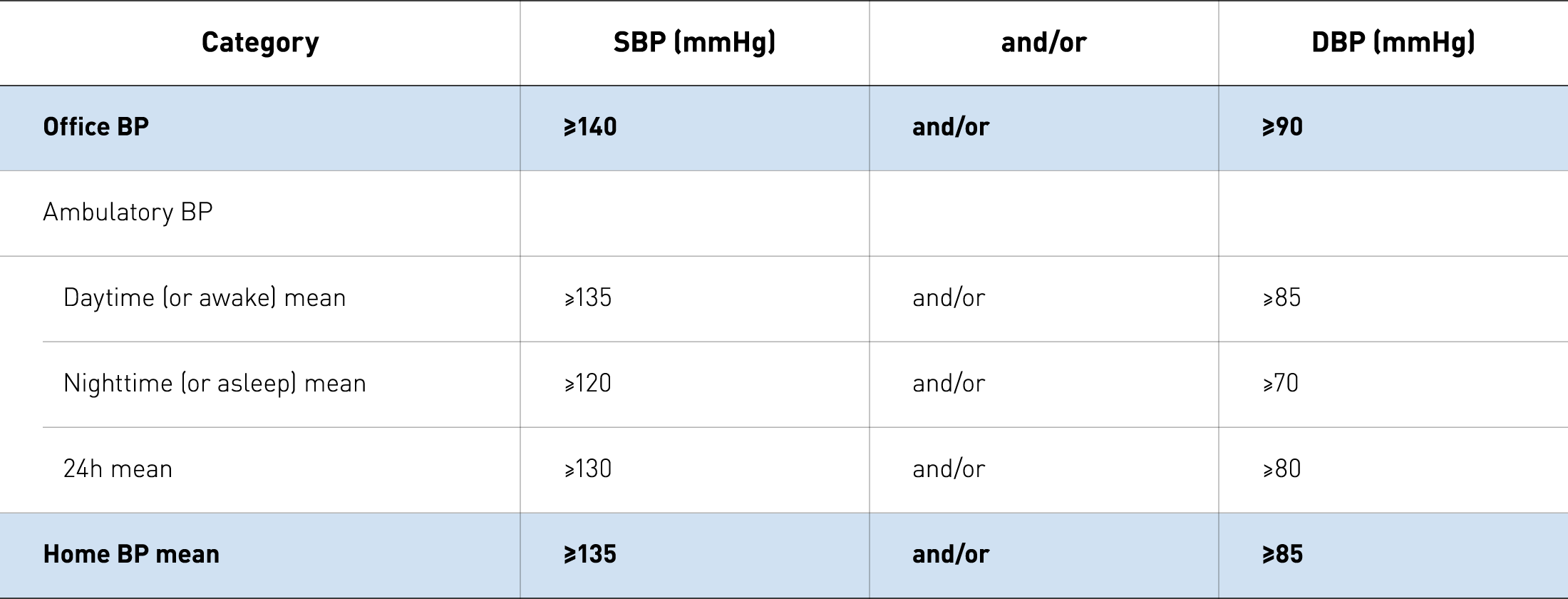
Definitions of hypertension according to office, ambulatory, and home blood pressure levels Category²
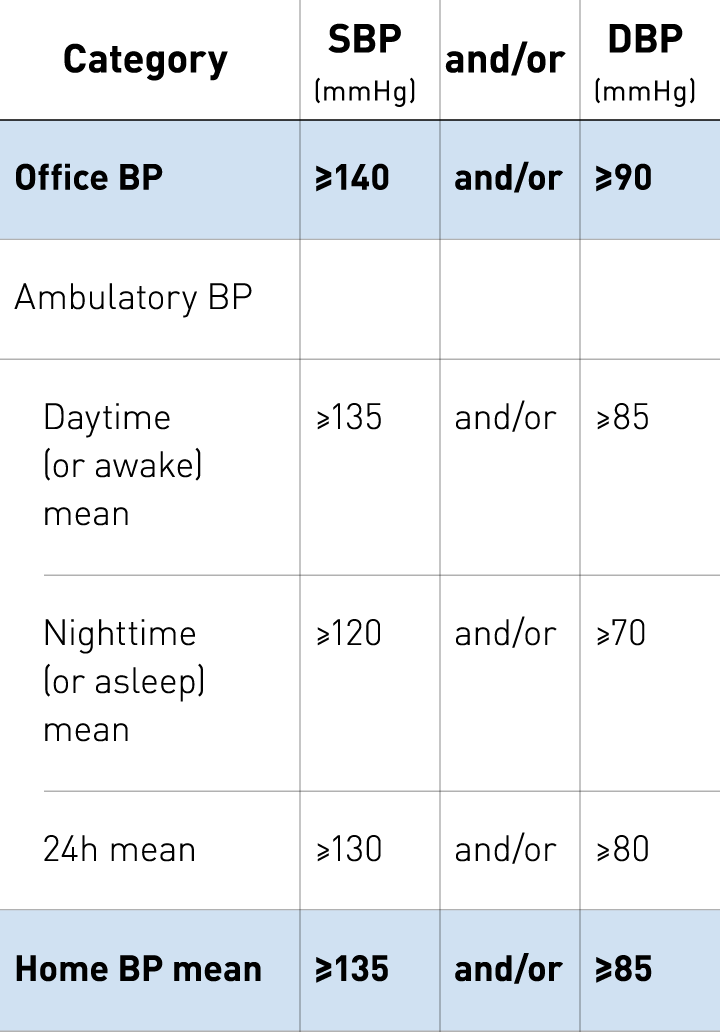
Definitions of hypertension according to office, ambulatory, and home blood pressure levels Category²
Masked hypertension: a systematic review⁴
The purpose of this research was to review the literature on masked hypertension. The prevalence of masked hypertension seems to lie between 8 and 20% and can be up to 50% in treated hypertensive patients. Subjects with masked hypertension have a higher risk of cardiovascular events than normotensive subjects. This is due to a possible failure to recognize and appropriately manage this form of hypertension, the frequent association with other risk factors and coexisting target organ damage.
White-Coat Hypertension – New Insights from Recent Studies⁵
White-coat hypertension indicates individuals who are not on treatment for hypertension but who had elevated office blood pressure and normal daytime blood pressure measured with ambulatory blood pressure monitoring (ABPM). Clearly, these individuals would be at low cardiovascular risk. The purpose of this review is to provide new insights into the characteristics, definitions, and cardiovascular risk assessment in persons with white-coat hypertension, and it will be limited primarily to ABPM with a primary focus on prospective studies.
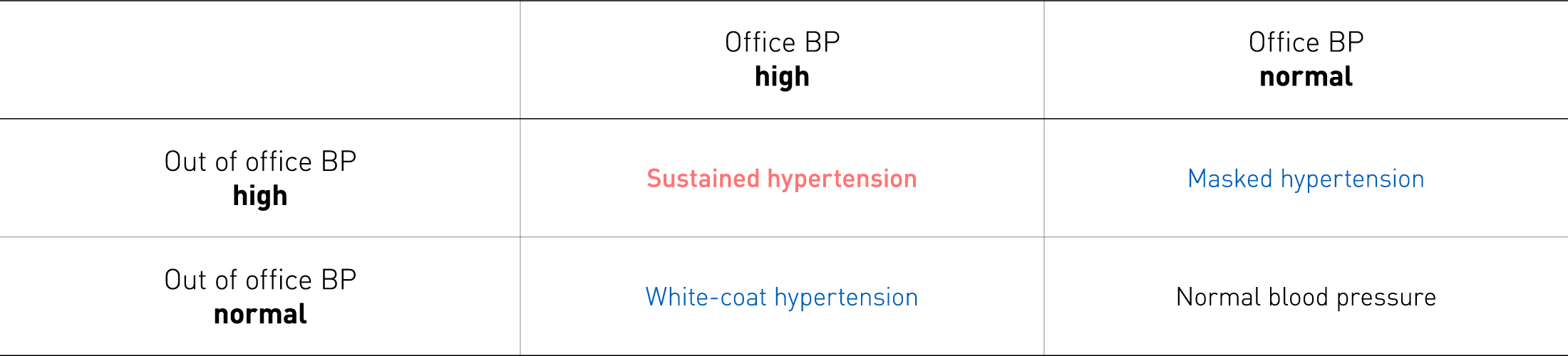
What is missed at the doctor’s office?²
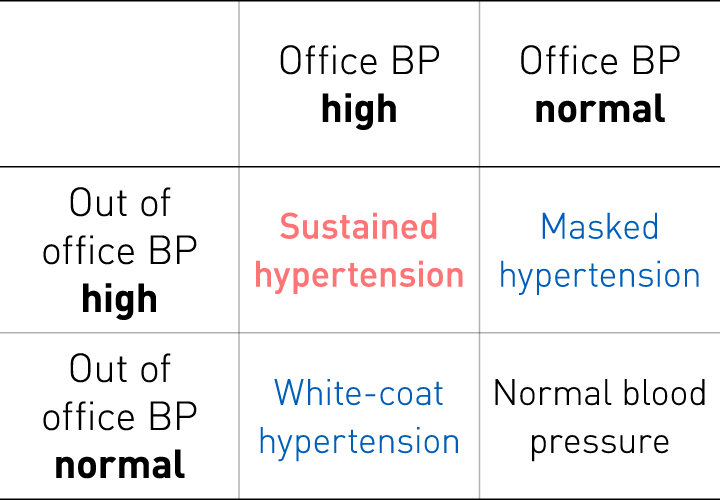
What is missed at the doctor’s office?²
OMRON’s Hypertension Plus
Supports clinicians to manage hypertensive populations more effectively.
Hypertension Plus includes unique clinical decision support tools based on NICE Guidelines and know-how from the TASMINH clinical trials. Guiding clinicians on when to act, and to provide a remote patient monitoring solution.

